Travel Reference
In-Depth Information
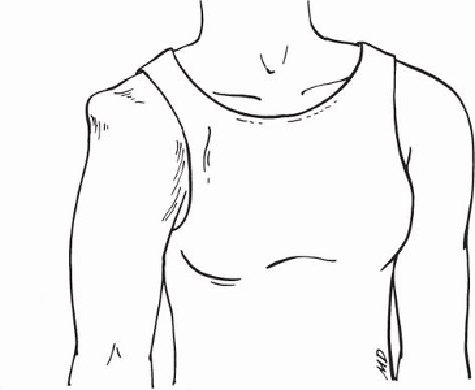
Figure 11-10. Appearance of a shoulder after anterior dislocation
Posterior shoulder dislocations are rare and often difficult to diagnose. The forearm and
upper arm are typically held across the chest in contact with the chest wall. The forearm
cannot be externally rotated away from the chest. A defect is usually present in the normal
contour of the deltoid muscle, which forms the outer point of the shoulder, and the head of
the bone in the upper arm (humerus) sometimes can be palpated posteriorly.
Ofthemanymethodsforreducingadislocatedshoulder,twoappeartocombinethebest
chance for success with the least risk of additional injury.
The first uses active traction by an attendant (
Fig. 11-11
)
. The person should be lying
flat with the injured arm held straight out from the side of the body. (A table for the indi-
vidualtolieonwouldprovidethebestpositioning,butawildernesssituationwouldrequire
improvisation,suchasalogorstonebench.)Theinjuredarmshouldbeflexedatfrontview
side view DISLOCATED the elbow and the forearm held in a vertical position. A loop
of webbing, clothing, or similar material that has been tied loosely around the attendant's
waist should be slipped over the arm and down to the elbow. After padding the elbow, the
attendant can apply traction by simply leaning backward. Another attendant must hold the
person, preferably with a loop of clothing around the chest, to prevent traction moving the
entire body.
Search WWH ::

Custom Search