Travel Reference
In-Depth Information
The signs and symptoms of hemothorax are similar to those of pneumothorax: im-
mediate pain, increasing difficulty in breathing, signs of decreased oxygenation (cyanos-
is—purple or bluish discoloration of the mucous membranes lining the mouth, lips, skin,
and nail beds due to reduced amounts of oxygen bound to circulating red blood cells—and
increased pulse rate), and absence of breath sounds over the involved lung. A large hemo-
thorax can eventually produce signs of shock due to blood loss. However, an observer can
seldom differentiate a hemothorax from a pneumothorax in the wilderness.
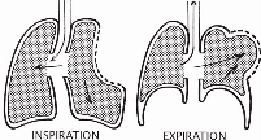
Figure 9-6. Pulmonary function with a flail chest
3
In fact, individuals may have both air and blood within the pleural cavity: a hemopneu-
mothorax. Only a chest X-ray can determine accurately what has accumulated. In either
case, the person must be evacuated. Hemothorax is treated initially the same as pneumo-
thorax, including supplemental oxygen.
Flail Chest
A flail chest is a condition produced by fracture of a number of adjacent ribs in two
or more places that produces a mobile, freely floating plate of chest wall that moves back
and forth during respiration. When the chest expands, the loosened segment of chest wall
moves inward. During expiration the loosened plate is forced outward: paradoxical respir-
ation. Since the chest wall moves without moving air into or out of the lungs, respiratory
distress results, even if the damaged area is relatively small (
Fig. 9-6
).
The individual usually has received a severe blow to the chest and is fighting for air
and breathing very rapidly. His lips, skin, and nails may be cyanotic due to reduced oxy-
gen availability. Examination of the bare chest discloses a mobile segment of chest wall
that moves paradoxically with each respiration. A simple fractured rib produces pain with
breathing but does not interfere with the movement of air.
The loosened segment must be immobilized. In an emergency, the individual should be
placed on the injured side (despite the pain) with a rolled-up piece of clothing beneath the
loose segment of rib cage (
Fig. 9-7
). The pressure effectively immobilizes the loosened
portion of the chest wall and allows more effective respiration. More secure fixation of the
rib cage can be achieved by taping or bandaging a large pad firmly over the mobile area,
but the dressing should be confined to the involved side of the chest.
Search WWH ::

Custom Search