what-when-how
In Depth Tutorials and Information
formation in advancing disease. The subtalar joint is more vulnerable
because of its complexity, vulnerable supporting structures, and its pivotal
role in walking. Structurally, the clinical manifestations are valgus deforma-
tion of the rearfoot, usually accompanied by medial longitudinal arch
collapse, and this is estimated to occur in 67 per cent of patients with
RA.
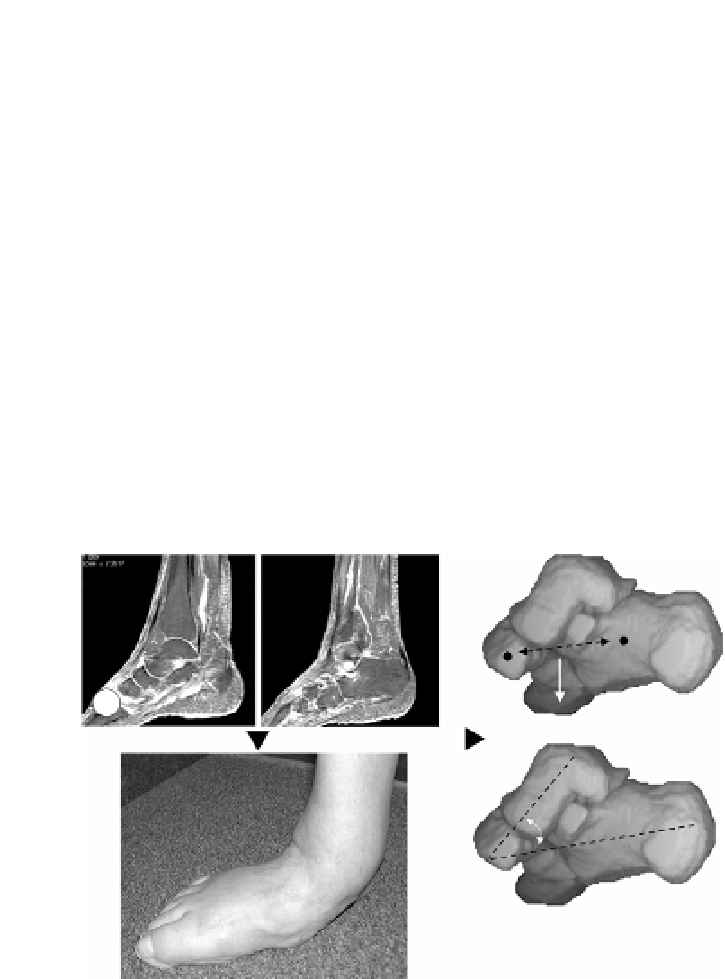
Dysfunction of the tibialis posterior tendon has been associated with
severe pes planovalgus deformity (
Figure 2.5
) in relation to the presence
of tenosynovitis, longitudinal tears and rupture.
Progressive deformity is associated with increased disease duration,
and pathology in the ankle and tarsus, with synovitis, tenderness and pain.
Platto et al (1991)
demonstrated significant gait impairment in RA
patients with rearfoot pain and valgus deformity. The appearance of
valgus heel deformity, medial longitudinal arch depression and bulging of
the talonavicular complex are often sufficient to clinically diagnose a
hyperpronated foot. The talonavicular joint inflammation and deformity
have an important and potentially contributory role to play in the develop-
ment of foot deformity (
Woodburn et al 2002
).
In addition to synovitis in the subtalar and talonavicular joints, the
forefoot joints are often affected. Daylight sign is the classic picture of
A
C
B
figure 2.5
Severe pes planovalgus deformity associated with RA. A - Two sagittal slices of
a post- gadolinium MR sequence showing disease activity in the tarsal joint region
B - the clinical picture of severe pes plano valgus deformity
C - 3D rendition of the calcaneus, cuboid, talus and navicular