Information Technology Reference
In-Depth Information
EEG in epilepsy. By choosing such apparently “long” segments we have been able
to detect spatiotemporal changes of dynamics over time that lead to prediction of
epileptic seizures tens of minutes ahead of their onset, at a respectable degree of
sensitivity and specificity [10, 11].
17.2.1.1 EEG from Barrow Neurological Institute, Phoenix, Arizona
Patient 1 was a 6-year-old patient admitted to the Epilepsy Monitoring Unit at
Barrow Neurological Institute, St. Joseph's Hospital, Phoenix, AZ. The EEG was
recorded with a standard International 10-20 scalp electrode montage (see Fig. 17.1)
at an A/D rate of 400 Hz. At the beginning of the recording, the EEG was charac-
terized by continuous ictal discharges associated with SE stage III and progressed
into ictal discharges punctuated by periods of flattening characteristic of SE stage
IV. During the EEG recording of SE, the attending physicians administered two
AEDs. The first AED (diazepam 10 mg) was administered rectally at 18 min into the
recording; the second AED (lorazepam 0.1 mg/kg) was administered intravenously
at 54 min into the recording. The proprietary EEG data were converted into 16-bit
signed binary format for further off-line nonlinear dynamical analysis.
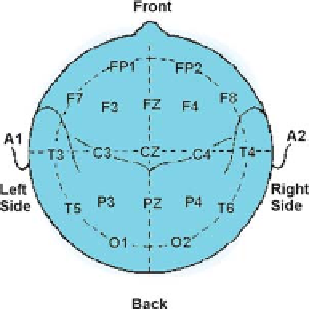
Fig. 17.1: Schematic diagram showing a standard scalp electrode placement, ac-
cording to the international 10-20 system as seen from above the head. A
=
Ear
lobe, C
=
central, P
=
parietal, F
=
frontal, Fp
=
frontal polar, O
=
occipital.
17.2.1.2 EEG from Mayo Clinic Hospital, Scottsdale, Arizona
The patient from this medical center (Patient 2) was a 75-year-old male with no his-
tory of seizures, brought to the emergency department after he was found unrespon-
sive at home with his right arm twitching and his head deviated to his right. When
the patient arrived at the emergency department he was observed having rhythmic