Information Technology Reference
In-Depth Information
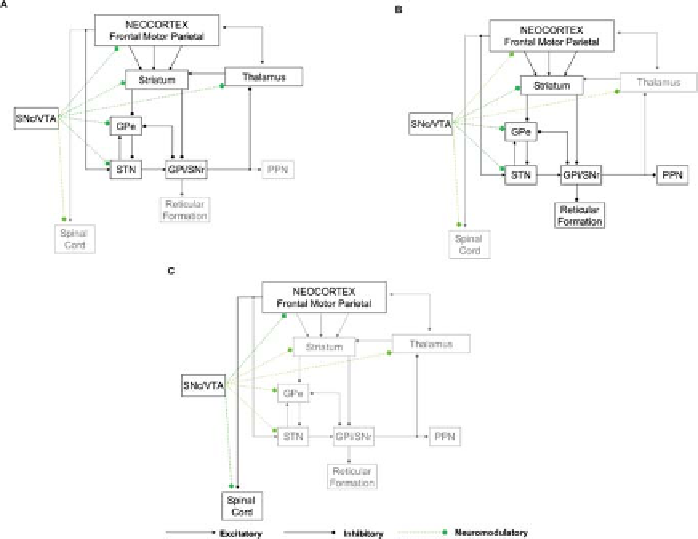
Fig. 11.1: Brain anatomical pathways in Parkinson's disease. (
A
) Pathways from
the substantia nigra pars compacta (SNc) and the ventral tegmental area (VTA)
to the striatum and from there to the thalamic nuclei and the frontal cortex through
the substantia nigra pars reticulata (SNr) and the globus pallidus internal segment
(GPi). (
B
) Pathway from the SNc and the VTA to the striatum and from there to
the brainstem through the SNr and GPi. (
C
) Pathway from the SNc/VTA to corti-
cal areas such as the supplementary motor area (SMA), the parietal cortex, and the
primary motor cortex (M1), and from there to the spinal cord.
the SNc/VTA to cortical areas such as the supplementary motor area (SMA), the
parietal cortex, and the primary motor cortex (M1), and from there to the spinal cord.
The most popular view is that cortical motor centers are inadequately activated
by excitatory circuits passing through the basal ganglia (BG) [1]. As a result, inad-
equate facilitation is provided to the otherwise normally functioning motor cortical
and spinal cord neuronal pools and hence movements are small and weak [1]. Re-
cently, a new view has been introduced by the modeling studies of Cutsuridis and
Perantonis [21] and Cutsuridis [18, 19, 20]. According to this view, the observed de-
layed movement initiation and execution in PD is due to altered activity of motor
cortical and spinal cord centers because of disruptions to their input from the basal
ganglia structures and to their dopamine (DA) modulation. The main hypothesis
is that depletion of DA modulation from the SNc disrupts, via several pathways,