Biomedical Engineering Reference
In-Depth Information
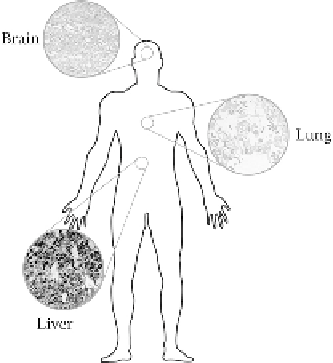
FIGURE 19.2
NP entry route into the body via the lung, particle accumulation in the liver, and the most
vulnerable site: the brain. (Reprinted with permission from Elsaesser A, Vyvyan Howard C. Toxicology of
nanoparticles.
Advanced Drug Delivery Reviews
. 2012;64(2):12-137.)
Aggregated silver NPs and some other nanomaterials have been shown to be cytotoxic to alveolar
macrophage cells as well as epithelial lung cells [29].
Another potential exposure route in humans is via the skin [30]. The skin is a structured organ
comprising three layers: the epidermis, the dermis, and the subcutaneous layer. The strongly kera-
tinized stratum corneum acts as the primary protecting layer and may be the rate-limiting barrier
to defend against the penetration of most micron-sized particles and harmful exogenetic toxicants.
Skin exposure to nanomaterials can also occur during the intentional application of topical creams
and other drug treatments [26]. Nanocrystalline magnesium oxide and titanium dioxide applied to
dermatomed human skin (as dry powder, water suspension, and water/surfactant suspension) for
8 h did not show dermal absorption through human skin with intact functional stratum corneum.
Whereas, titanium dioxide (TiO
2
) NPs having a size range of 20-100 nm, when topically applied
in porcine-, healthy human-, and human-grafted skin samples, get restricted to the topmost 3-5
corneocyte layers of the stratum corneum. However, TiO
2
particles could get through the human
stratum corneum and reach the epidermis and even dermis. Flexing movement of normal skin was
shown to facilitate the penetration of micrometer-sized fluorescent beads into the dermis [31]. The
quantum dots (QDs) could penetrate the intact stratum corneum barrier and get localized within the
epidermal and dermal layers [32]. In a clinical study, treatment of burns using nanosilver-coated
dressings led to abnormal elevation of blood silver levels and argyria (blue or gray discoloration
of the skin due to silver accumulation in the body over time which is a “cosmetic problem”) [33].
The nanosilver-based dressings and surgical sutures have received approval for clinical application
and good control of wound infection is achieved. However, their dermal toxicity is still a topic of
scientific debate and concern. The nanocrystalline silver-coated dressing is more cytotoxic among
the cultured keratinocyte extracts of several types of silver-containing dressings. Fullerene-based
peptides are capable of penetrating into the intact skin [34]. Intradermally administered QDs could
enter subcutaneous lymphatics [35] and regional lymph nodes [36]. Topically applied fine and
ultrafine beryllium particles can be phagocytosed by macrophages and Langerhans cells, possibly
leading to perturbations of the immune system [31]. Epidermal keratinocytes are capable of phago-
cytosing a variety of engineered NPs and setting off inflammatory responses [37]. Some other types
of NPs, such as single-/multiwalled carbon nanotubes (SWCNTs, MWCNTs), QDs with surface
coating and nanoscale titania, may produce toxic effects on epidermal keratinocytes and fibroblasts.
They are capable of altering their gene/protein expression [38].