Biomedical Engineering Reference
In-Depth Information
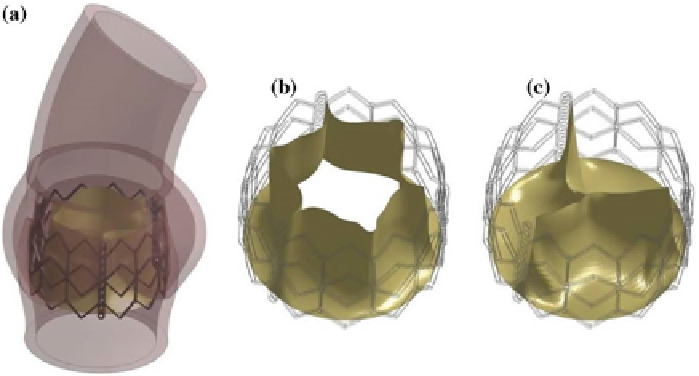
Fig. 8 a
TAV leaflet in model P2 after positioning simulation,
b
TAV model at early systole and at
c
late diastole
4 Discussion
TAV implantation are currently considered a feasible procedure in high risk and
inoperable patients affected by severe aortic stenosis [
27
]. The current indications
still limit TAV to a minority of clinical cases, while it can be claimed that moderate
and low risk patients could also benefit from TAV advantages (i.e. avoid general
anesthesia and the trauma deriving from SAVR, possibility to perform valve-in-
valve implantation) [
5
]. The assessment of TAV in lower risk patients is still far to
come, but the potentials of this endovascular approach are promising. In this context
computational methods and tools could play an important role in supporting clinical
investigations, as well as the process of device design, with the aim of improving
TAV performances and overcome its current limitations and critical aspects.
Having this in mind, in this paper a FE approach for the simulation of both the
implantation and function of a TAV model was described: the approach was applied
to three MRI-based AR models in which the degree of AV stenosis differed, ranging
from absence of calcific stenosis (model H), typically observed early calcifications
(model P1) and extended calcifications on the commissural zones of the AV (model
P2).
To the best of our knowledge, the proposed modeling approach is the first one
that accounts for both native AV leaflets and TAV leaflets and that analyses the
post-implantation scenario throughout the cardiac cycle. Moreover, in the developed
FEMs the anisotropic and non linear behaviour of the native AV, as well as the non
linear mechanical response of the TAV pericardium leaflets was included.
The analyses allowed to investigate how the degree and location of AV calcifi-
cations could affect TAV performances: indeed, a distortion in the post-implanted