Biology Reference
In-Depth Information
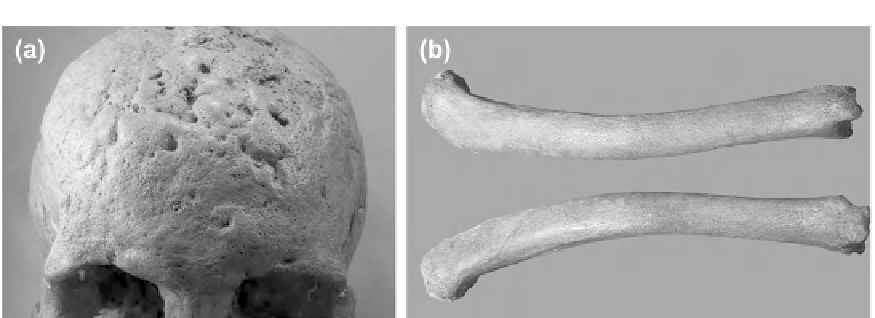
FIGURE 7.4
(a) Pathognomonic caries sicca of treponemal disease. (b) Diagnostic sabre tibiae of treponemal
disease.
screening is now possible and the genetic markers for brucellosis have bridged this diag-
nostic gap (
Mutolo et al., 2012
). Indeed, genetic data have confirmed tuberculosis and plague
(Yersinia pestis) in other circumstances (e.g.,
Crub´zy et al., 1998; Mays et al., 2001; Verena
et al., 2011
) and may become a more common paleopathologic diagnostic tool in the future.
Non-venereal Treponemal Disease
Non-venereal treponemal disease
8
is a chronic infectious cutaneous disease of childhood
transmitted by skin-to-skin contact. It has an antiquity of 3000
years (as yaws and/or tre-
ponarid) in North America (
Powell et al., 2005
). Like tuberculosis, it is a disease of aggregate
living and poor community hygiene that became pervasive in North American skeletal
samples with the intensification of agriculture (Powell and Cook, 2005).
Treponemal disease often presents as nondiagnostic periostitis, but it also has distinctive
reactive changes that are pathognomonic for the disease (
Hackett, 1975
). These include cavi-
tating lesions on the cranium that heal in a star-shaped (stellate) pattern and, in an advanced
state, coalesce to a nodular (coral or cauliflower textured) cranial surface (known as caries
sicca) (
Figure 7.4
a). Diagnostic of treponemal disease is a marked anterior bowing of the tibia
(sabre shins) (
Figure 7.4
b). Nasopalatal damage is also characteristic of non-venereal and
venereal (i.e., syphilis) treponemal disease.
This type of damage is also characteristic of leprosy (or Hansen's disease) (
Cook, 2002
), an
illness of considerable antiquity and profound social stigma (
Zias, 2002
; Roberts, 2002;
Robbins et al., 2009; Stone et al., 2009
). However, leprosy is not indigenous to the NewWorld.
Distinguishing leprosy from syphilis rests diagnostically on the former's predilection for
distal body elements (hands and feet). These display as contracted and atrophied (claw
hand appearance) or atrophy of the distal fingers and toes (pencil point appearance) (Aufder-
heide and Rodr
´
guez-Mart
´
n, 1998;
Ortner, 2003
).
Themore observations that canbemarshaled, the greater the likelihood a deduceddiagnosis
is the correct one. That is, zeroing-in on the primary or most extensive pathological condition is
þ
8
The venereal form, syphilis, is not unequivocally evident in pre-Columbian Europe and apparently of
North American origin but of unclear antiquity (Powell and Cook, 2005).