Biology Reference
In-Depth Information
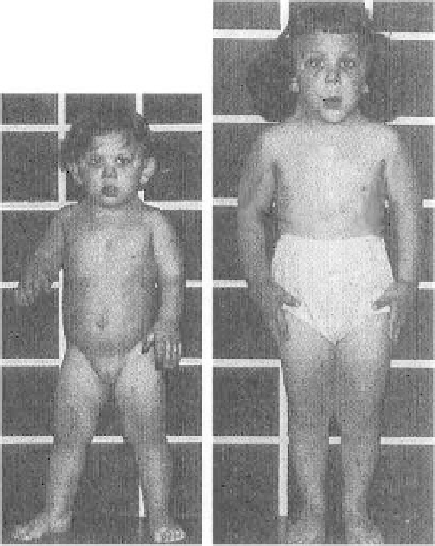
FIGURE 5.4. Girl with Turner syndrome at ages 2 and 4 years. Notice large, promi-
nent ears, webbed neck, and short staure (Jones 1997, with permission of W.B.
Saunders Co.).
microdeletion syndromes exist that give rise to recognizable genetic disor-
ders. Among these are the DiGeorge/velocardiofacial syndromes, which
usually result from a deletion in chromosome 22 in band q11, and the
Prader-Willi/Angelman syndromes, which are most often caused by dele-
tions of chromosome 15 in bands q11-q13. Deletions in some disorders are
large enough to be seen on a routine karyotype, but molecular techniques
such as fluorescence in situ hybridization (FISH), where fluorescently
labeled DNA probes are hybridized to chromosome spreads, have become
the standard for diagnosis of these disorders.
The clinical phenotype resulting from a chromosomal deletion can be due
to loss of one critical gene, or to a set of contiguous genes. For example,
Alagille syndrome is characterized by ocular, skeletal and cardiac defects
in association with loss of intrahepatic bile ducts. Additional anomalies may
also be present. A large deletion of chromosome 20p12 is observed in
several families with Alagille syndrome; however, point mutations in the
gene Jagged1 (
JAG1
), which maps to this locus, also cause the same syn-
drome (Li et al. 1997; Oda et al. 1997), suggesting deletion of only this one
gene is sufficient to cause the syndrome. In contrast, Miller-Dieker syn-