what-when-how
In Depth Tutorials and Information
ICF-CY
Part 1
FUNCTIONING/
DISABILITY
Part 2
CONTEXT
Component 1
BODY
Component 2
ACTIVITIES/
PARTICIPATION
Component 3
ENVIRONMENTAL
FACTORS
Component 4
PERSONAL
FACTORS
Component
level
Body
Functions
Body
Structures
1
st
level
8 chapters
8 chapters
9 chapters
5 chapters
2
nd
level
118 cat.
56 cat.
132 categories
74 categories
3
rd
level
351 cat.
166 cat.
394 categories
185 categories
54 cat.
99 cat.
17 categories
9 categories
4
th
level
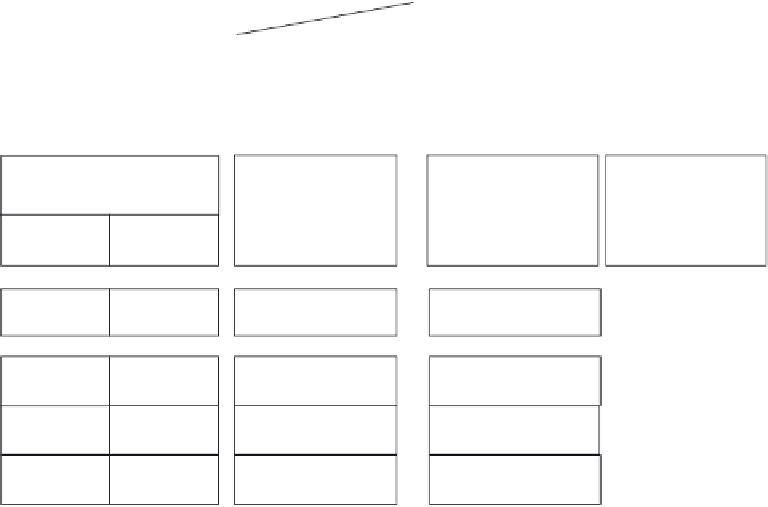
FIGURE 51.1
The hierarchically nested structure of the WHO International Classification of Functioning, Disability and Health, version for
Children and Youth (ICF-CY).
8
ICF-CY could serve as a conceptual model. All func-
tional outcome measures described in this chapter are
divided in three categories: (1) body function and struc-
ture; (2) participation and activities and (3) outcome
measures and utilized instruments.
Furthermore, the role of intervention and physical
training, next to perspectives for current and future
clinical diagnostics and treatment strategies within
the domain of functional outcome, are described and
discussed.
Engelbert et al. underlined these cross-sectional find-
ings in their prospective study, in which children with
OI type I decreased significantly in total joint ROM
(especially in the lower extremities) and generalized
joint hypermobility (median Bulbena score at the start
7.5 and at follow-up 6;
p
-value <0.001) after a 4-year
follow-up period.
10
However, in OI types III and IV, a
severe decrease in total joint ROM was present without
significant changes over time. This latter was explained
by the authors as due to the biomechanical skeletal
properties within the more severe OI types.
10
BODY
FUNCTION AND STRUCT
URE
Muscle Strength
Muscle strength is a health-related fitness component
and refers to the ability of the muscle to exert force.
11
Although decreased muscle strength can be clinically
seen in children with OI, the etiology of muscle weak-
ness in these patients is relatively unclear but may be
due to an intrinsic muscle defect.
12
Studies regarding
muscle strength in this specific population are relatively
scarce and muscle strength is mostly described as an
element in studies assessing physical function or the
effects of (non) pharmacological interventions.
Some of the earlier studies describing muscle strength
in children with OI are by Engelbert et al. in which semi-
quantitative scores (manual muscle testing) were used
to determine muscle strength (cross-sectional) in a large
Range of Joint Motion
The cross-sectional study of Engelbert et al. indi-
cated that range of joint motion (ROM) of children with
OI type I (not treated with medication) was approxi-
mately analogous to healthy references.
9
Furthermore,
generalized joint hypermobility was reported in 17 out
of 24 children with OI type I. Children with OI type III
showed a severe decrease in joint ROM, especially pro-
nounced in the proximal joints of the extremities (shoul-
der and hip joint), in which the lower extremities showed
a more pronounced decrease of ROM compared with
the upper extremities. This same study also indicated a
decreased ROM in children with OI type IV, especially
shown in the lower extremities.
9