what-when-how
In Depth Tutorials and Information
growth, the rods slide away from each other (
Figure 45.2
).
This technique seems to be more difficult to use than tele-
scopic rods
6
but remains cheaper than telescopic rodding
and is still used in countries where budget constraints
limit the use of more expensive implants.
In 1987, Metaizeau proposed the use of the elastic
nail (Nancy nail) instead of Rush pins for sliding rod-
ding, but the mid-term results were not very promising
particularly for children older than 5 years of age.
7
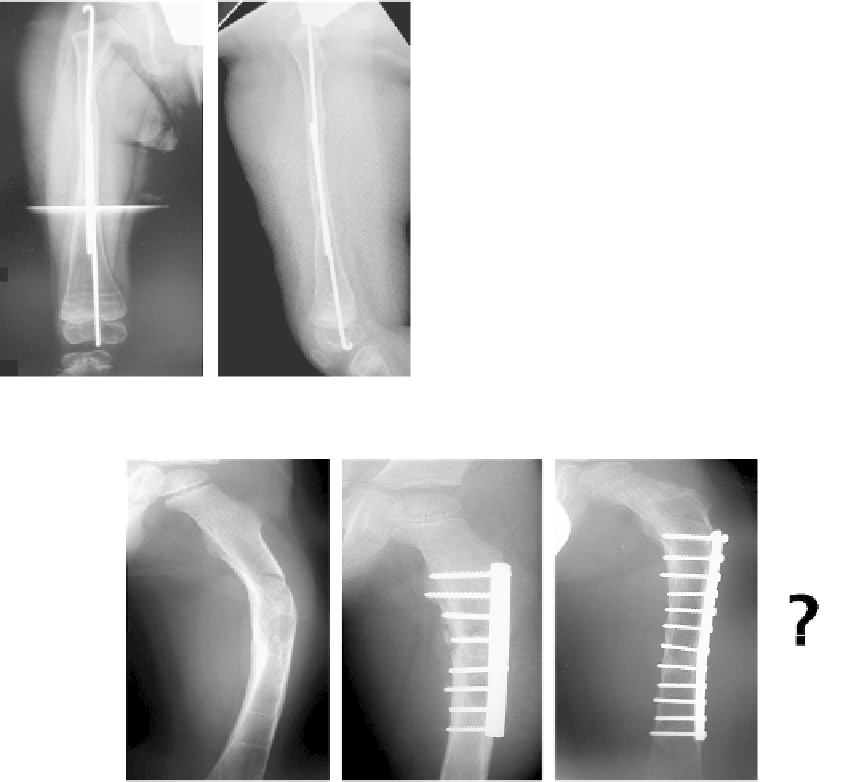
However, the bones remain brittle and the results of
using plates remain poor.
9
Therefore, rodding remains
the best choice for the fixation of OI bones (
Figure 45.3
).
RODDING OF OI BONES
Rodding of OI bones still presents several unan-
swered questions and solutions to these questions are
still under debate:
1.
What material should be used: stainless steel or
titanium?
So far, because of the bone fragility, titanium rods
(elastic rods or Nancy nails) seem to be too elastic and
the tutor effect of the rod is more or less ineffective
due to the flexibility of the nail. It is used in Europe
though but the results do not demonstrate
10
better
outcomes than regular stainless steel rod.
11
In addition, the use of an elastic rod (as it is curved)
at the time of insertion (to provide mechanical
stability) creates false tracks in OI bone during
surgery. When used as a “sliding rod” system, it
loses the benefit of the “belly” and the mechanical
stability is compromised.
2.
How to choose the size of the rod?
It would be logical, from a mechanical standpoint,
to use the largest possible rod with regards to the
diameter of the shaft of the bone. But OI bone does
not have the shape of a normal bone, and it is often
“rib-shaped” meaning that the bone is flattened with
a large diameter in the frontal plane (plane of the
deformity) but a very small diameter in the sagittal
plane. The sagittal plane is the most important
diameter to consider when choosing the size of the
implant. Intra-operatively, there is always a strong
temptation to ream “another size up” to insert a
bigger rod, but OI children need more bone than
metal and therefore this should be avoided.
A
ROD. WHY NOT A PLATE
?
As early as 1982,
8
the poor results and the many com-
plications of plates in OI bones have been reported. Acting
as a stress riser, the plate creates a very rigid segment, and
the (abnormal) bone is likely to break above or below the
plate. Recently, with the observation that with bisphospho-
nates the bone was stronger, it was felt that perhaps plates
could be used. (Better purchase for the screws.)
FIGURE 45.2
Sliding rods.
FIGURE 45.3
Femoral fracture treated with a plate. Following a new fracture below the plate, the surgeon chose to use a longer plate. A rod
would have been a better option.