what-when-how
In Depth Tutorials and Information
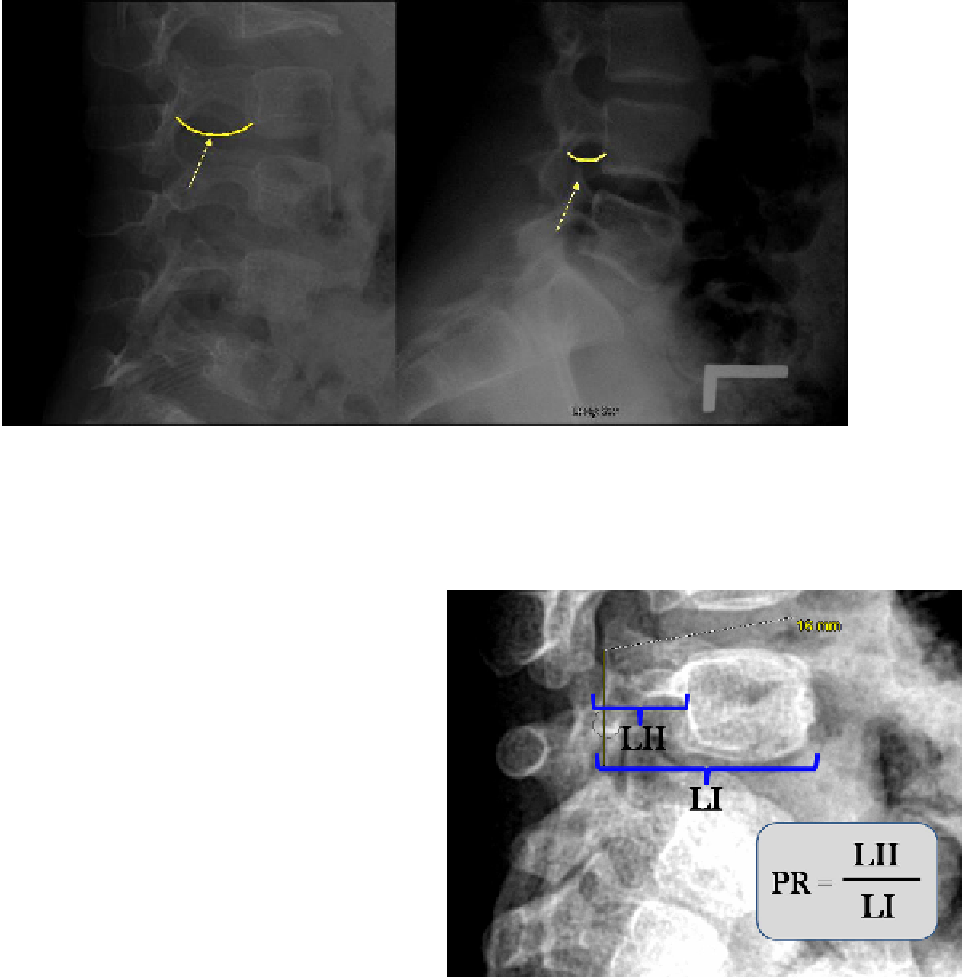
FIGURE 44.15
Normal pedicle length on the right with a child with type I OI. On the left is the elongated pedicle length in a child with a
more severe form of OI. It is unknown if bisphosphonate treatment has any effect on this length, but some individuals can have spondylolisthe-
sis from pedicle elongation alone which can occur over time with progressive elongation of the pedicle.
(Reproduced with permission from Wolters Kluwer Health)
all were treated with bisphosphonates and, where indi-
cated, surgical realignment and intramedullary stabili-
zation of their extremities was performed.
17
Hatz also noted the abnormal elongation of the ped-
icles in 40% of their patients, essentially all in children
with the more severe forms of OI (
Figure 44.15
). They
attempted to develop a means to measure this abnor-
mality and recognize the difficulty in doing this with-
out a valid control group (
Figure 44.16
).
17
This finding
has been noted previously by other authors.
38,39
Ambulatory children with OI have a tendency
to a significantly increased lumbar lordosis with an
increased pelvic incidence at the lumbosacral junc-
tion. There are limited data on the sagittal alignment
in children with OI, however.
49
The exact reason for
this increased lumbar lordosis in children with OI is
unclear, as clinically many of the children do not have
hip flexion contractures or other significant sagittal
malalignment on standing lateral radiographs or clini-
cal examination. This particular finding has not been
extensively studied, although there have been efforts to
define the spinal structure and alignment in individu-
als with OI. The authors postulate that individuals with
OI are predisposed to repetitive hyperextension stress
injuries not only from this increased lumbar lordosis,
but also because of the relative weakness of their bone
structure. Historically, individuals with type III and IV
OI had limited ambulatory ability and thus were not
predisposed to spondylolysis and spondylolisthesis.
With aggressive medical management, and surgical
alignment of their lower extremities, they are clearly
more active than historical cohorts, and this likely leads
FIGURE 44.16
Pedicle length ratio. Some individuals with the
more severe forms of OI will have elongated pedicles relative to the
length of the vertebral body.
(Reproduced with permission from Wolters Kluwer Health)
to a higher incidence of spondylolysis and spondylolis-
thesis. It is also likely, in the authors' opinion, that the
incidence of lysis and listhesis is actually higher than
reported by Hatz et al. The relative osteoporosis and
limited ability to visualize the involved area adequately
on limited plane radiographs can make interpretation
difficult. If CT or MRI studies were to be performed,
which are not usually clinically indicated, it would be
anticipated that significantly more posterior element
abnormalities would be diagnosed.