what-when-how
In Depth Tutorials and Information
CERVICAL SPINE
with treatment with halter traction and cervical collar
in the case reported by Rush.
33
It is obviously of great
concern that these individuals may develop cord com-
pression over time and require operative treatment, but
there is no guidance from the literature as to the opti-
mal treatment of this abnormality in patients with OI.
Paraplegia after chiropractic manipulation has also
been reported.
11
The cervical spine can obviously be involved with
subtle fractures, instability and cranial settling. The
treating physician must be acutely aware of the cranio-
cervical abnormalities that occur in OI, which are
covered in another chapter of this topic. This is espe-
cially true if the need for anesthesia is anticipated.
Stabilization of the neck by the surgeon at the time of
intubation and positioning in all patients is important
to prevent injury to the spinal cord, as many of these
abnormalities may be undiagnosed. Vertebral body
fractures can obviously occur in OI but in clinical prac-
tice, symptomatic or obvious cervical abnormalities
are less common than thoracic or lumbar fractures in
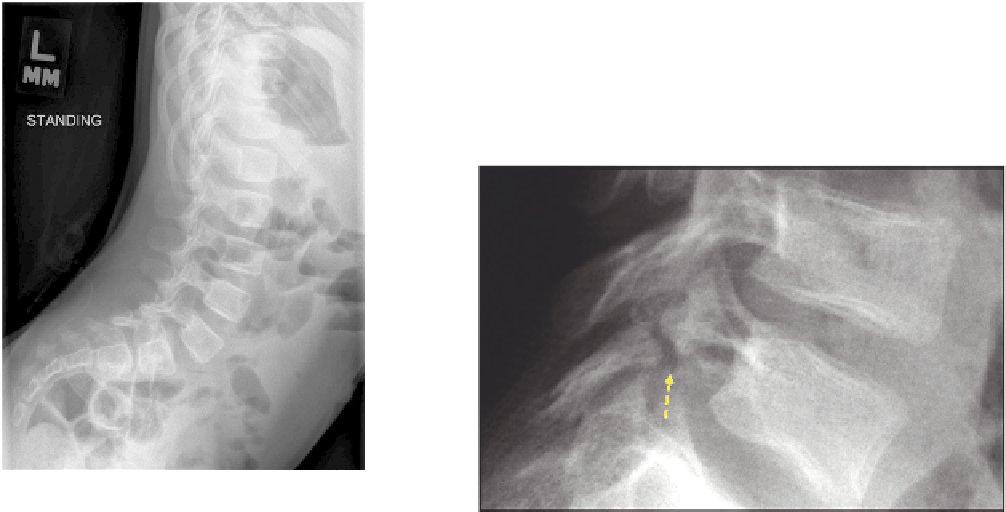
the authors' observation. The one fracture pattern that
has been noted in our clinic population in two patients
is a fracture or congenital abnormality of the posterior
elements of C2 or Hangman's fracture. One of these
patients with type III OI initially presented as a dys-
plastic elongation of the pars at age 2 years, 11 months
of age. He was treated with a cervical collar but by age
3 years, 10 months had a clear-cut lysis though remains
asymptomatic (
Figure 44.7A, B
). The second patient in
our clinic presented with an absence of the lateral mass
of C2 at 6 months of age and also continues to be asymp-
tomatic (
Figure 44.8A, B
).
Three-dimensional CT (
Figure 44.8C, D
) scan veri-
ies the space between the lamina and body of C2 with
absence of the lateral mass. A similar fracture healed
SPONDYLOLYSIS AND
SPONDYLOLISTHESIS
Spondylolysis is a defect in the pars interarticularis of
the vertebrae. This typically occurs in the lower lumbar
spine, most commonly at L5-S1 because of the increased
stress on the posterior elements due to lordotic posture
at that level (
Figure 44.9
). It does not typically occur in
individuals who do not ambulate. There are a variety of
classifications of spondylolysis.
34,35
The most common
type seen in OI is isthmic, which is felt to be secondary
to multiple repetitive stresses on a potentially predis-
posed individual (
Figure 44.10
). It is also more common
in individuals who perform repetitive hyperextension
activities. The second type that is most commonly seen
in OI patients is the dysplastic type.
34,35
This is caused by
an elongated, abnormally formed pars, which therefore
is weaker and more prone to failure. In OI, the predispo-
sition to spondylolysis may be related to a combination
of both factors (
Figure 44.11
).
36
It is also common to see
elongated pedicles, especially in patients with the more
severe types of OI, such as type III (
Figure 44.12
).
17,37-39
The incidence of spondylolysis in the normal popula-
tion has been reported to be 4.4% in the pediatric pop-
ulation, increasing to about 6% by adulthood.
34,35,40-43
Spondylolisthesis is described and defined as a forward
slippage of the vertebral body onto the vertebral body
FIGURE 44.9
Four-year-old with type IV OI with the increased
lumbar lordosis and anterior pelvic tilt seen in many ambulatory chil-
dren with OI. Note also the elongation of the lumbar pedicles and
pars with mild listhesis of L5 on S1.
FIGURE 44.10
Isthmic spondylolysis.