what-when-how
In Depth Tutorials and Information
(A)
(B)
(C)
(D)
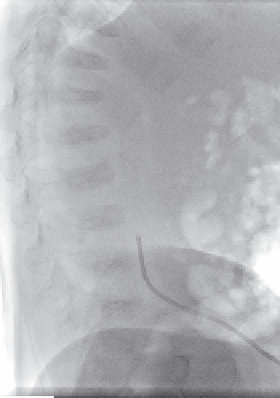
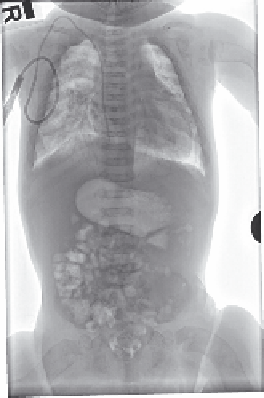
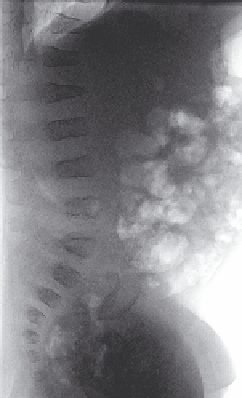
FIGURE 44.3
(A, B) Anterior posterior and lateral spine X-rays of a 2-month-old child with type IX OI (homozygous mutation in the PPIB
gene). Subtle codfish vertebral changes L2 with wedging of essentially all other vertebrae. (C, D) Follow-up Anterior posterior and lateral X-rays
at 8 months of age showing improved vertebral height of the lower lumbar vertebrae and improvement in the contour of the vertebral end plates.
vertebral disc is stronger than the vertebral body.
23
The
central portion of the vertebral body essentially col-
lapses around the disc, while the cortical margins of the
vertebral body are relatively maintained.
1-3,14,18,24
The
codfish vertebra has been noted to be present in many
individuals with severe scoliosis.
2,3
The vertebra can
also be flattened, or can have a wedge or compressed
type pattern (
Figure 44.3
). Ishikawa reported that in his
series six or more biconcave vertebrae before puberty
were predictive for the development of scoliosis, but
that biconcave vertebrae did not appear to affect the
severity of kyphosis.
14
The codfish vertebra is well rec-
ognized and described most commonly in the more
severe forms of OI. It is difficult, however, to deter-
mine if there is a specific type of OI associated with this
deformity. This is complicated by the fact that the older
literature used varying classification systems of OI,
18,24
which cannot be clearly correlated with the modified
classification of Sillence,
25
including the recognition of
the atypical types of OI which are being identified with
improved diagnostic techniques. It is clear, however,
that those with more severe forms of OI have more
fractures and that more secondary deformity occurs in
these individuals.
1-3,14,18,24
Standardized X-ray views
26
and further study of the sagittal balance in children
with OI need to be further defined and standardized
to determine the specific patterns of deformity and the
effectiveness of treatment.
27,28
Aström et al. studied the effect of treatment on spi-
nal development in infants and young children treated
with pamidronate, with the initial treatment at an aver-
age of 3.6 months of age. These individuals had docu-
mented vertebral fractures that were not present in the
neonatal period. They showed a slow but significant
increase in the vertebral height, as well as improved
vertebral morphology and bone density as they fol-
lowed them over 3-6 months of treatment. The histori-
cal age-matched control group of children who were
not treated with IV pamidronate but had comparable
forms of OI demonstrated progressive and worsening
deformity.
6
Similar improvements have been described
by others.
5,7,8
It is much less common now to find a
child with persistent codfish vertebrae in an OI clinic
population who is treated early in life with bisphospho-
nates and with optimization of diet and activity.
It is well recognized clinically that individuals with
residual deformity and OI have significant functional
problems as adults, with progression of kyphoscoliosis
and back pain into adulthood.
29,30
Thus, it is imperative
to treat individuals early in life with optimized medi-
cal management to maintain vertebral height and shape
(
Figure 44.4
). Reconstitution of vertebral height in older
children or adults has not been as common or predict-
able following bisphosphonate treatment.
5-8
Treatment of vertebral fractures must be individu-
alized to the patient because of the variability of pain,
deformity and inability to tolerate orthotic treatment
(
Figure 44.5
). Acute neurologic injury can occur but has
rarely been described in the literature.
12
In very young
infants and children, many times these fractures occur
with minimal trauma and may be minimally symp-
tomatic. A short period of rest and analgesics is often
associated with the prompt return to baseline activi-
ties and comfort. Orthotic treatment does not appear to
improve ultimate alignment, and can be associated with
deformity of the ribs and chest wall.
2,4
However, treat-
ment with bisphosphonates may improve bone strength
to the point that orthotic treatment can be considered