what-when-how
In Depth Tutorials and Information
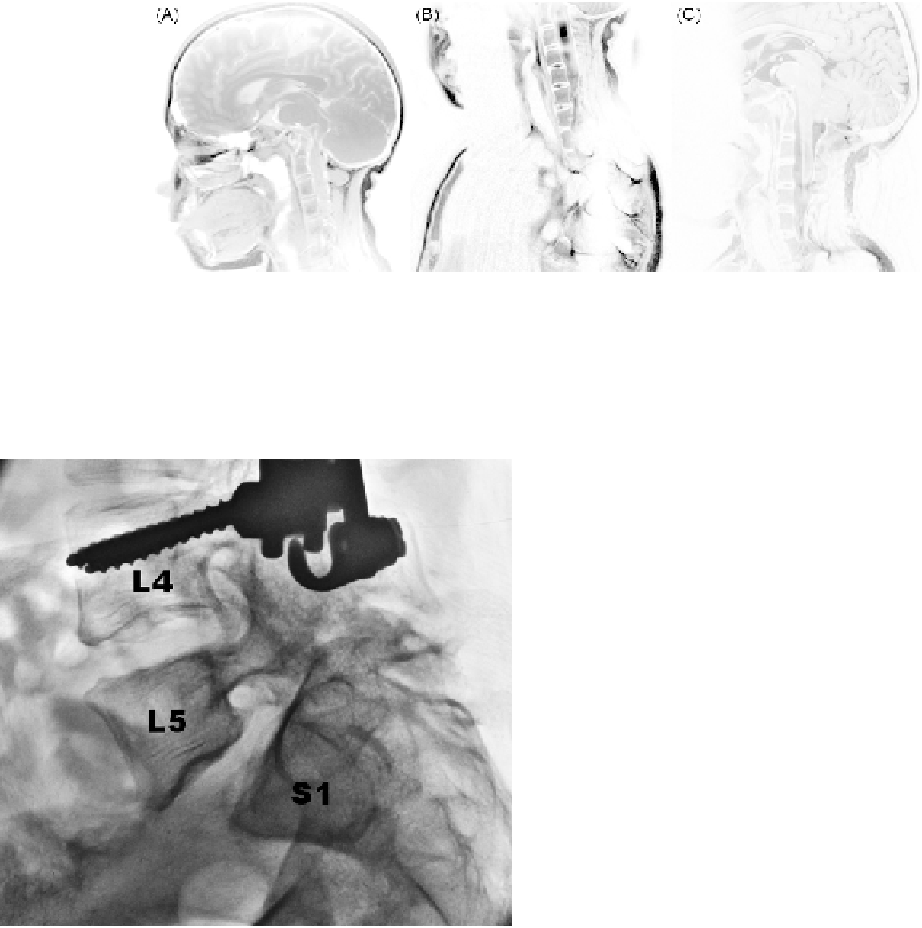
FIGURE 43.1
MRI images showing the pathology of an OI patient with basilar invagination. (A) Preoperative sagittal T1-weighted image
shows evidence of basilar invagination, narrowing of the foramen magnum, and compression of the anterior surface of the medulla oblongata
resulting in neurologic symptoms on examination. (B) Preoperative sagittal T2-weighted image demonstrates a multiloculated syringomyelia
in the cervical cord extending from C2 through at least C6. (C) Following upper cervical laminectomy with dorsal occipitocervical fusion, this
T2-weighted image demonstrates resection of the anterior arch of C1 and partial resection of the body of C2 (odontoid process) with relief of the
cord compression.
the vertebra below, usually following spondylolysis.
Both conditions are typically found in the lower lum-
bar spine, a direct result of increased stress on the pos-
terior elements of the lordotic spine. Deformation of the
bone from the increasing mechanical load that naturally
occurs during childhood can cause rapid progression of
hyperlordosis and pedicle elongation resulting in spon-
dylolisthesis and spondylolysis.
9,10
Although there have been many case reports and iso-
lated findings, the incidences of spondylolysis and spon-
dylolisthesis have not been frequently estimated in the
literature. The few studies that investigated these con-
ditions have demonstrated higher prevalences of these
conditions in OI patients as compared to the general pop-
ulation. A study by Hatz et al. observed a spondylolysis
incidence of 8.2% and a spondylolisthesis incidence of
10.9% in pediatric OI patients.
11
As a comparison, normal
children below the age of 6 have a spondylolysis inci-
dence of 4.4%, which increases to 6% in the adult popula-
tion.
12
Spondylolisthesis incidences range from less than
3% in children to 6-8% in adults.
13
The Hatz study noted that their observed incidence
of spondylolysis was higher than a reported figure of
5.3% in a study by Verra et al. Interestingly, 79% of the
patients included in the Hatz study were capable of
holding themselves upright to some degree, which con-
trasted with the Verra study, where none of the patients
were capable of ambulation or significant physical activ-
ity. This suggests that OI patients who are capable of
ambulating are more prone to developing spondyloly-
sis and spondylolisthesis. This is most likely a result of
an increased load-bearing requirement of the lumbar
spine in ambulating patients. Lastly, Hatz qualitatively
observed that many of the ambulatory patients included
in the study had increased pelvic incidence and hip con-
tractures, which can lead to further stress on the lumbar
spine.
11,14
FIGURE 43.2
OI patient with spondylolisthesis. One can observe
anterior subluxation of L5 on S1. Pedicle screws from the fusion con-
struct are seen in L4.
The subject of craniocervical junction abnormalities
is discussed in greater detail in Chapter 36 (see Basilar
Invagination), which includes further information on
diagnosis and treatment.
SPONDYLOLISTHESIS AND
SPONDYLOLYSIS
Spondylolisthesis and spondylolysis are spinal con-
ditions that are relatively unique to bipedal ambulators.
Spondylolysis is a defect or break in the pars interar-
ticularis of a vertebra. Spondylolisthesis (
Figure 43.2
)
is the forward movement of one vertebra relative to