what-when-how
In Depth Tutorials and Information
has been reported by Kim et al.
15
In ten patients with
transient osteoporosis of the hip the T-1 MRI signal
intensity of the femur trochanter was compared to the
proximal femoral metaphysis. The proximal femoral
metaphysis was isointense (fatty marrow) relative to
that of the greater trochanter. This study suggested that
the conversion of hemopoetic to fatty marrow in the
proximal femur altered intramedullary blood low to
the hip resulting in edema.
Stress fractures are a likely etiology for TMO in any
joint or following the stress of pregnancy. Trevisan
16
reported findings in three men, aged 30-50 years, who
complained of several episodes of arthralgia in the
lower limbs, with a migratory pattern and radiographic
evidence of focal osteoporosis. These individuals dem-
onstrated severe systemic osteoporosis with prominent
trabecular involvement. The authors suggested that a
prolonged or exaggerated activation of “regional accel-
eratory phenomena (RAP)” is the cause of transient
osteoporosis. Bone tissue microdamage due to osteo-
porosis was suggested as the cause of microfractures.
The concept of regional acceleratory phenomena was
initially formulated by Frost who stated that under
“noxious tissue stimuli” the ordinary regional biologi-
cal processes, including blood low, cell metabolism and
turnover, and also tissue modeling and remodeling,
may be greatly accelerated in specific foci leading to
microdamage.
17
This concept would now be expanded
to include the release of damaging cytokines, e.g., IL-6,
TNF-α and perhaps others that would accelerate bone
turnover and increase the likelihood of microdamage.
In OI individuals, a susceptible joint may suffer
stress fractures due to the combination of strain on a
joint where bone mass is inherently weakened. Joint
strain involving the hip, knee or ankle may result from
previous fractures with resultant deformity leading to
stress patterns around the joint. Altered gait would be
one potential source of joint stress.
Although stress fractures may lead to bone edema,
TMO may be associated with clinically apparent frac-
tures. Miyanishi et al.
18
reported that radiographs
obtained 2 months after the onset of hip pain in a
45-year-old male showed a focal loss of radiodensity
in the left femoral head. MRI revealed bone marrow
edema with an associated subchondral serpiginous
low signal intensity line on the T1-weighted images.
A CT scan showed a subchondral fracture. However,
this occurrence is not typical of TMO in which the con-
tours of the femoral head remain intact.
In OI, localized bone edema is usually not a feature
of long bone or vertebral fractures. However, the occur-
rence of a migratory pattern in certain patients and
during or following pregnancy suggests that factors
in addition to the injury
per se
act to induce changes in
several joints. Consistent with the multi-joint involve-
ment in the inflammatory arthropathies, a suggestion
would be that perhaps following stress fractures with
the release of inflammatory cytokines such as IL-6 or
TNF-α, a process would be established which could
promote involvement of other joints. However, the
release of inflammatory peptides in TMO has not been
reported.
BONE HISTOLOGY AND CLINICAL
L
ABORATORY TESTS IN TM
O
The results of core bone biopsies of the involved fem-
oral trochanter-neck-head and iliac crest in a 48-year-
old woman with type I OI and transient osteoporosis
were reported by Noorda et al.
19
The iliac crest biopsy
showed increased surface extent of osteoid seams but
was not diagnostic of osteomalacia. However, there
was an increase in the numbers of osteoclast resorp-
tion lacunae. The histologic pictures were consistent
with a high turnover state. Biopsy of the involved
femur head showed bone marrow edema, a reduced
number of thin bony trabeculae with small break lines
in trabeculae suggesting microfractures. Bone biop-
sies from 19 patients with transient regional osteo-
porosis were examined by McCarthy. All but one
case showed marrow edema which appeared as pale
esoinophilic material between marrow fat cells (
Figure
39.2
). This material was occasionally foamy. Six cases
showed small lipid cysts but fat necrosis was not pres-
ent. Fourteen cases showed thin seams of woven bone
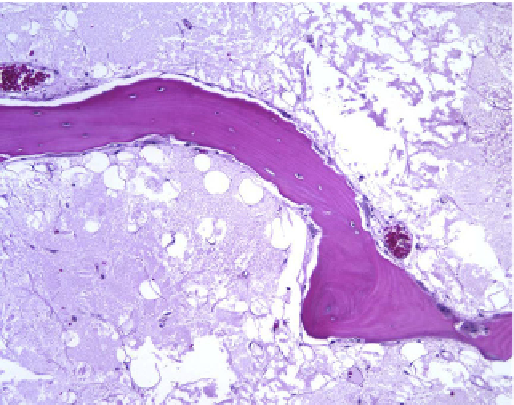
FIGURE 39.2
Bone histology in transient edema: trabecular bone
is diminished. One lamellar segment is illustrated. There is accumu-
lation of foamy cells in the region of trabecular bone.