what-when-how
In Depth Tutorials and Information
developmental defect cannot be reversed or lessened
once they are formed.
7
The fact that orthodontic movement was not
achieved or could be limited in the OI types IV and III
dentition hinders future planning. It is recommended
that the child see an orthodontist by age 7 years to
check for a developing open-bite and/or Class III
malocclusion. The developing Class III malocclusion
with maxillary hypoplasia is most efficiently treated
by orthodontic and orthopedic jaw movement at this
approximate age,
74
although the lack or delay of erup-
tion of the permanent maxillary first molars makes the
use of an attached palatal expansion appliance with a
reverse facemask difficult if not impossible. The influ-
ence of the bisphosphonates and their long half-life in
the bone matrix further complicates predicting results.
A summary of “Dental Care for Persons with OI” may
be viewed and downloaded from the website of the
Osteogenesis Imperfecta Foundation. The current
URL for the summary is
http://www.oif.org/site/
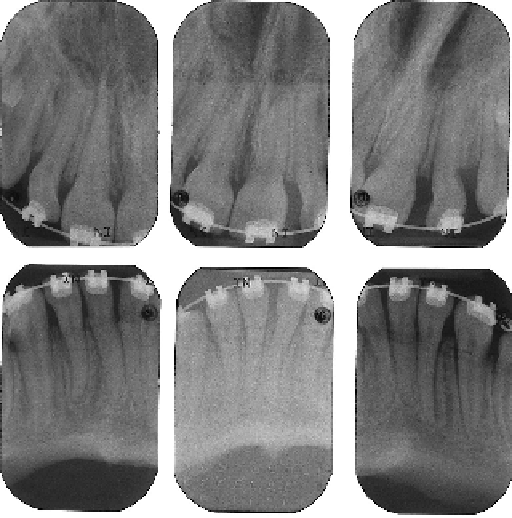
FIGURE 33.19
Periapical radiographs of an OI type III patient.
After 18 months of treatment and slow orthodontic movement, no
evidence of root resorption is evident.
References
These variable developmental defects exist in the
teeth of all patients with OI, regardless of whether DI
is clinically visualized or not.
14
But the tooth is not the
only oral anatomical structure that is so affected. All
tissue that contains type I collagen would be expected
to be affected at least on a microscopic developmen-
tal level.
6
It is recommended that children see a pedi-
atric dentist by 6 months after the eruption of the first
baby tooth. Regular dental care is needed so the teeth
will last as long as possible and to prevent abscesses
and pain. Brushing and cleaning has not been shown
to cause damage, but will not make teeth affected by
DI white. Sealants should be effective on teeth affected
with DI as long as the enamel is intact.
13
The origins of these dental defects, as well as the
unusual prevalence of malocclusion, are not completely
understood. It is apparent that some of the pleiotropic
effects of the type I collagen that yields the variable
manifestations of OI may also be similarly produced by
mutations in other genes (e.g., DI secondary to muta-
tions in the
DSPP
gene not as a part of OI; and PFE
secondary to some
PTHR1
mutations). Further investi-
gation of the interactive developmental and functional
pathways that form mineralized tissue may ultimately
yield a better understanding of the development of the
anomalies and their primary treatment.
Unlike bone, enamel and dentin tissues do not
remodel. Therefore, their shape and any dentin
[10]
[11]