what-when-how
In Depth Tutorials and Information
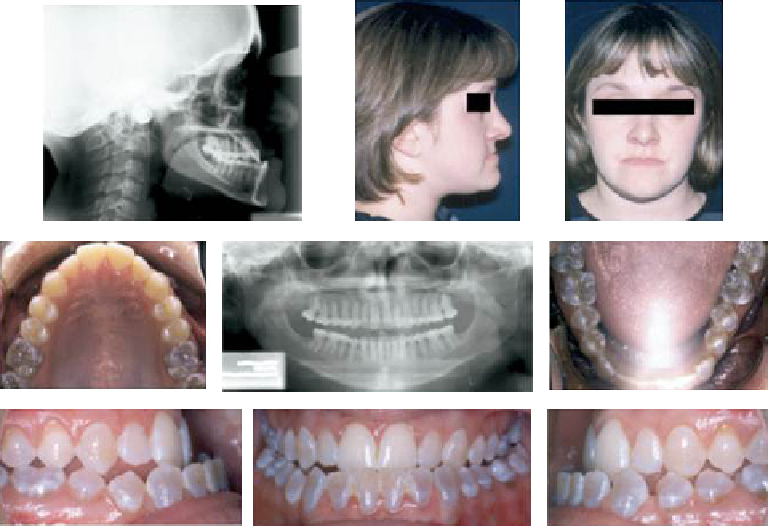
FIGURE 33.14
Adult with type IV OI with mandibular prognathism (Angle Class III malocclusion), and DI.
(From ref.
48
)
degree the type I patients, it can be said that it repre-
sents the norm in this particular population, and will
need to be addressed to treat the malocclusion and
maximize the masticatory and speech functions of OI
type III and IV patients (
Figures 33.14 and 33.15
).
56
dentoalveolar structures and the condylar process were
identified as the main reasons for the relative man-
dibular prognathism in OI.”
52
These characteristics are
normally not found in the general population and rep-
resent much more challenging malocclusions to treat
than most.
Lateral open-bites have been reported to be
extremely rare and affect less than 1% of a sample.
69
This condition is overrepresented in the OI population,
affecting 27% of type III patients, and up to 33% of type
IV patients.
54
These open-bites tend to be extremely
severe and probably dramatically impair the chewing
capabilities of the OI patients who have them. The eti-
ology of these open-bites may be caused by the lack of
vertical descent and development of the dentoalveolar
processes.
70
Non-functional posterior lateral cross-bites are also
a prevalent aspect of OI dental malocclusions. In the
normal population, posterior cross-bites are normally
caused by a slightly reduced width of the maxilla occlud-
ing with a normally developed mandible.
71
Scalia et al.
have demonstrated that posterior cross-bites on OI
patients, unlike that generally found in the general popu-
lation,
71
are non-functional and are actually caused by an
enlarged mandibular dentoalveolar process, especially in
the molar area (
Figure 33.16
).
55
The etiological factors for
this condition are not well understood, although a lower
than normal tongue position exerting pressure on the
dentoalveolar process combined with a wider and longer
mandible are potential contributing factors.
Difference in Severity of Malocclusions between
Types of OI
In order to evaluate the degree of malocclusion
presented by OI patients when compared to non-OI
patients in need of orthodontic treatment, Rizkalah
et al. used the DI and PAR indexes of malocclusions
to assess the differences in severity of a malocclusion
of the OI population.
54
Another study conducted by
Carbone et al. (submitted for publication) looked also at
the DI index of OI patients in relation to matched con-
trols.
68
From both studies the OI population presented
a much higher index of malocclusion severity than the
non-OI untreated or group of patients seeking ortho-
dontic treatment. The DI index obtained on a matched
untreated sample was 6.33, while the DI index of the
OI sample was 29.6.
68
Rizkalah et al. had reported a DI
index of 12.4 for a population in need of orthodontic
treatment, also vastly smaller than in the OI sample.
54
An overrepresentation of Class III malocclusions,
as well as the presence of severe lateral posterior
open-bites that are rarely seen in normal populations,
point to the specificity of the malocclusions presented
by OI patients. “Vertical underdevelopment of the