what-when-how
In Depth Tutorials and Information
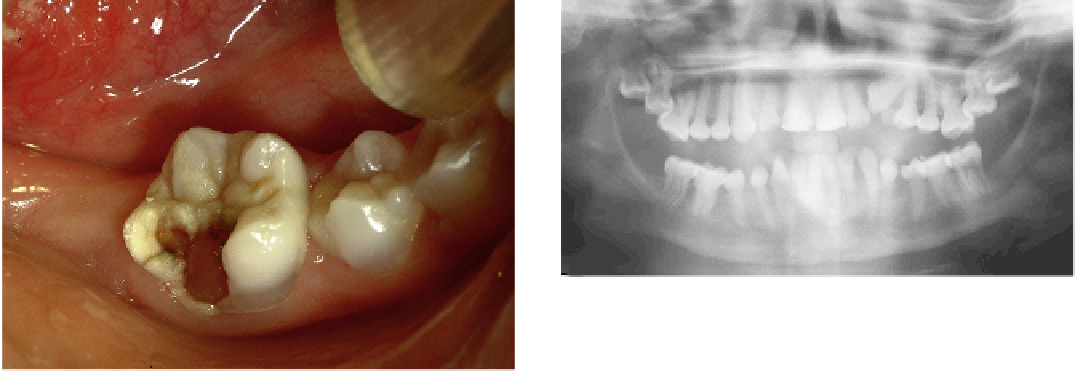
FIGURE 33.4
The pan-oral radiograph shows the bulbous crowns
of the teeth with calcified canals. The child is 14 years old. The man-
dibular second molars have just erupted and have large pulpal
spaces. Pulpal spaces calcify very quickly once they erupt. The pulpal
spaces of the maxillary second and third molars are wide and the
molars are impacted.
FIGURE 33.2
Spontaneous fracture of a permanent molar with
DI. Notice the color of the underlying dentin.
immediately after the eruption of the teeth. For some
unknown reason denticles and abnormal dentin are
constantly laid within the pulp.
16
This process is rapid,
and pulps of the DI teeth seem to achieve total oblitera-
tion before adulthood.
Periodontal Ligament (PDL)
Fibroblasts are the principal cells of the PDL. They
have the particularity of being able to produce colla-
gen at an exceptionally high rate. At its formation, the
ligament space is occupied by loose connective tissue
connecting the root with the supporting bone. Then,
the ligament fibroblasts produce collagen bundles
that establish the strong anchorage of the tooth. The
ligament fibroblast is a unique cell, capable of simul-
taneously synthetizing and degrading collagen.
17
Furthermore, the contractile proteins in its cytoskeleton
allow it to move. The fibroblast can pull itself forward
or remain stationary and pull in adjacent elements by
using its contractile forces. It is definitely involved in
the tooth eruption because the force needed to move a
tooth is linked to the contractibility of fibroblasts.
FIGURE 33.3
The primary incisor on the left belongs to a child
with OI. The primary incisor on the right belongs to a healthy child.
However, not all OI patients have teeth that are smaller than normal.
OI teeth may be small (
Figure 33.3
). They all have a
bulbous crown that is particularly constricted at the
cemento-enamel junction.
3,9,14
Ameloblasts and odon-
toblasts determine the shape of the crown at an early
stage of its development, and the genes expressed dur-
ing this stage are associated with DI, dentin dysplasia
and amelogenesis imperfecta (odontoblasts: CO1A1,
COL1A2 and DSPP; ameloblasts: AMELX, ENAM,
MMP20 and KLK4).
15
Some authors suggest that the
exaggerated bulging of the crown is responsible for
the impaction of some permanent molars (
Figure 33.4
).
Different hypotheses are offered further on.
The constriction of the DI posterior teeth appears
even more striking because of the roots' slenderness
that accentuates its demarcation from the crown.
16
The
development of the roots are initiated once the crown
is completed. Pulpal spaces begin showing during or
The Erupting Tooth Movement in Health and in DI
During root formation, the elongation of the root
corresponds to the increase of the jaw's vertical dimen-
sion, and one might erroneously conclude that the two
events are related. It is known that roots will continue
forming even when the teeth do not erupt, such as in
cleidocranial dysplasia.
18
However, the roots may be
twisted and short in OI type III or IV patients (
Figure
33.5
). The presence of the dental follicle, the capability
of the bone to model and the behavior of the fibroblasts
are all intimately accountable for tooth eruption.
6,19
In order for a tooth to emerge into the oral cav-
ity, extensive bone modeling must take place and the