what-when-how
In Depth Tutorials and Information
were added to this model, the correlation between serum
25-hydroxyvitamin D levels and lumbar spine areal
BMD z-scores were no longer significant, suggesting that
the effect of 25-hydroxyvitamin D levels on lumbar spine
areal z-scores was mediated by parathyroid hormone
concentrations.
This study suggested that raising 25-hydroxyvitamin
D levels could help to increase lumbar spine areal BMD
z-scores in young OI patients.
19
The regression equation
in that study indicated that for every 1 nmol/l increase
in 25-hydroxyvitamin D levels, lumbar spine areal BMD
z-score increased by 0.008. Thus, the effects on lumbar
spine areal BMD z-scores that could be achieved with
higher vitamin D intake are probably relatively modest
but considering the generally good safety profile of vita-
min D, additional supplementation might still be useful.
This hypothesis is tested in ongoing randomized con-
trolled trials.
HI Girls
HI Boys
Helical
α
1 Girls
Helical
α
1 Boys
Helical
α
1 Girls
0
Helical
α
1 Boys
-1
-2
-3
-4
-5
-6
-7
-8
0
2
4
6
8
10
12
14
16
18
Age (Years)
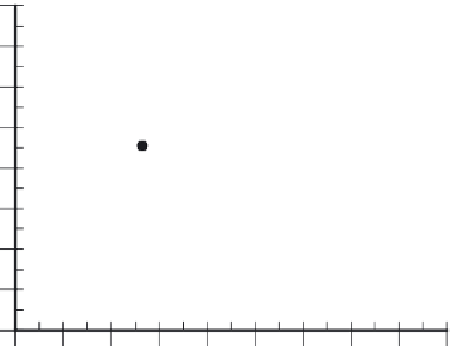
FIGURE 24.2
Age-dependency of lumbar spine areal BMD
z-scores in patients with
COL1A1
haploinsufficiency mutations (HI),
as well as with
COL1A1
and
COL1A2
mutations leading to glycine
substitutions in the collagen type I helical domain. Within each geno-
typic group, BMD varies widely, suggesting that factors other than
COL1A1
/
COL1A2
mutations play a role in determining BMD in OI.
(From: Rauch F, Lalic L, Roughley P, Glorieux FH. Relationship between
genotype and skeletal phenotype in children and adolescents with osteogen-
esis imperfecta. J Bone Miner Res 2010;
25
: 1367-74.)
BISPHOSPHONATE TREATMENT
EFFECTS ON BMD IN OI
Intravenous Bisphosphonates
Many studies have documented the marked increase
in areal BMD following the start of intravenous bisphos-
phonate treatment.
20-31
A more systematic investigation
of this observation was undertaken in a longitudinal
study which assessed the effect of 4 years of intravenous
pamidronate treatment on lumbar spine bone densito-
metric results in 56 children and adolescents with OI.
20
Results were compared to those of 167 patients who had
not received pamidronate prior to densitometry. In all
patients who received pamidronate, bone mass increased
above levels expected for untreated patients. After 4
years of treatment bone mineral content and volumetric
BMD were 154% and 65%, respectively, higher in than
in untreated patients who were matched for age and OI
type. This difference between bone mineral content and
volumetric BMD was explained by the fact that bone size
also increased more in the pamidronate-treated group.
Remarkably, the treatment effect could be observed in
every single patient, as each of the 56 patients on pami-
dronate treatment increased bone mineral mass faster
than expected in untreated patients.
The structural bone changes underpinning these
changes in BMD are likely to include an increase in cor-
tical thickness, as evidenced by both radiological and
histomorphometric analyses.
29,32
In addition, the relative
amount of trabecular bone tissue within the trabecular
compartment increases during pamidronate treatment,
due to an increase in trabecular number.
33
Another factor
likely to influence the increase in BMD during bisphos-
phonate treatment is the accumulation of calcified
are responsible for the higher lumbar spine areal BMD
values in girls. Bone histomorphometric observations
showed that bone turnover was lower in girls than in
boys. Lower bone turnover is expected to lead to slightly
higher bone mass, because at any one time a smaller
amount of bone will have been transiently removed by
remodeling. It is thus possible that lumbar spine areal
BMD is higher in girls with OI because their bone turn-
over is less elevated than that of boys.
Among patients with helical mutations, neither the
type of alpha chain affected, nor the type of amino acid
substituting for glycine, nor the position of the muta-
tion in the alpha chain had a detectable relationship
with lumbar spine areal BMD. Thus, there was no clear
genotype-phenotype correlation with regard to BMD
among patients with helical glycine mutations.
Vitamin D and Bone Mineral Density
Apart from the type of the disease-causing mutation,
vitamin D status is a putative determinant of BMD in
OI.
18
A cross-sectional study on 282 pediatric OI patients
found that serum 25-hydroxyvitamin D levels were posi-
tively associated (
P
= 0.02) with lumbar spine areal BMD
z-scores, after accounting for clinical OI severity, age
and gender.
19
When serum parathyroid hormone levels