what-when-how
In Depth Tutorials and Information
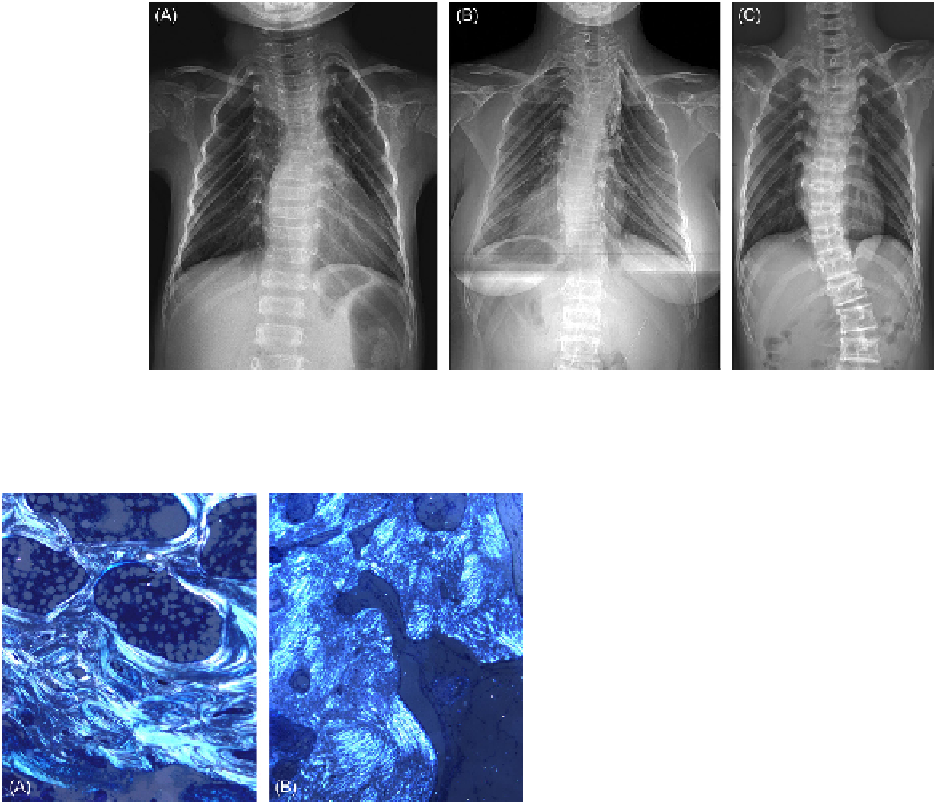
FIGURE 20.9
Vertical arrangement of the posterior ribs is a characteristic radiographic finding. (A, B) Narrow upper part and relatively
wide lower part forms a pyramidal or bell-shaped thoracic cavity. (C) Some patients show narrowing of both upper and lower parts of the tho-
racic cavity.
TH
ERAPEUTIC INTERVENTIO
NS
Cyclic intravenous pamidronate has a similar effect in
OI type V as in other types of OI. Initial febrile episode
is encountered as in other types, and then it decreases
urinary excretion of NTx, may cause mild hypocalcemia,
increases bone mineral density, decreases fracture fre-
quency, and improves ambulatory status.
27,43
Long bone stabilization for fracture or for deformity
correction can be achieved by intramedullary rod-
ding along with single or multiple osteotomy(ies) as
in other types of OI. The possibility of developing HC
should always be taken into consideration. Scoliosis
is not uncommon in OI type V as in other types of OI.
However, progression to a significant curve is not fre-
quent and spinal fusion is rarely indicated. A dislocated
radial head usually does not cause any functional dis-
turbance, and its surgical excision is indicated usually
for cosmetic purposes. It may be associated with lim-
ited elbow joint motion. However, other reasons for
joint stiffness such as subperiosteal bone formation
around the elbow joint (
Figure 20.7C and D
) should
also be considered since in that case radial head exci-
sion might not improve the motion in the elbow joint.
Pain syndrome associated with chronic or acute
subperiosteal bone formation is difficult to control. Non-
steroidal anti-inflammatory drugs, steroids or bisphos-
phonates do not seem to bring any symptomatic relief.
FIGURE 20.10
Polarized microscopic finding of the undecalcified
section from an iliac crest bone biopsy. (A) Lamellar pattern of the
haversian system from a normal subject. (B) Mesh-like lamellar pat-
tern in OI type V.
(Adapted from
30
with permission.)
contrasted from OI type IV whose lamellar arrange-
ment and appearance are well preserved.
1
In 1993,
Stöss et al. investigated uninjured bone tissue from OI
patients with HC using light and electron microscopes,
and reported that the collagen fibrils of the uninjured
bone tissue showed irregularities in their delimitation,
massive differences in diameter, and split ends in some.
This case is highly likely to be OI type V.
Conspicuous clinical and radiographic findings of, and
identification of causative gene mutations for, OI type V
make bone biopsy non-essential in the diagnosis of this
disease. Nevertheless, the histopathologic findings may
contribute to understanding the pathogenesis of OI type V.
Biochemical studies are usually non-specific, and
there are no abnormalities except for elevated serum
alkaline phosphatase level and urinary excretion of NTx
during the active phase of HC.
1,33,36,37
References